Why is treatment of a low sperm count so confusing ?
Many infertile men are obsessed about their sperm count - and this seems to become the central concern in their lives. Remember that the real question the man with a fertility problem is asking is not: What is my sperm count or motility or whatever? But - are my sperm capable of working or not? Can I have a baby with my sperm? Since the function of the sperm is to fertilize the egg, the only direct way of answering this question is by actually doing IVF for test fertilization. This is, of course, too expensive and impractical for most people which is why the other sperm function tests have been devised.
The major problem with all these tests, however, is that they are all indirect --- there is no very good correlation between test results, pregnancy rates, and fertilization in vitro for the individual patient. This is why offering a prognosis for the individual patient based on an abnormality in the sperm test result is so difficult, and why we find that different doctors give such widely varying interpretations based on the same sperm report.
This is really not surprising when you consider how abysmal our ignorance in this area is - after all, we do not even know what a "normal" sperm count is! Since you only need one "good" sperm to fertilise an egg, we do not have a simple answer to even this very basic question! While the lower limit of normal is considered to be 10 million progressively motile sperm per ml, remember that this is a statistical average. For example, most doctors have had the experience of a man with a very low sperm count (as little as 2-5 million per ml) fathering a pregnancy on his own, with no treatment. In fact, when sperm counts are done for men who are undergoing a vasectomy for family planning, these men of proven fertility have sperm counts varying anywhere from 2 million to 300 million per ml. This obviously means that there is a significant variation in "fertile" sperm counts, and therefore coming to conclusions is very difficult for the doctor (leave alone the patient!)
In order to make sense of this, you need to understand two important concepts - "trying time" and "fertility potential of the couple". If your sperm count is low, but you have been trying to have a baby for less than 1 year, it still makes sense to keep on trying for about 1 year, since 10% of men with low sperm counts will father a pregnancy in this time. If however, you have already tried for more than 2 years with no success, you need to move on and do something more - the chances of a spontaneous pregnancy are now very low. Remember, that a doctor does not treat just a "low sperm count report" - he treats patients!
What can the man with a low sperm count do ?
So what is the man with a low sperm count to do? Unfortunately, there is no method of increasing the sperm count today! The modern protocol for managing male infertility is based on the man's motile sperm count; and on a simple test, called a sperm survival test. The sperm are washed, and their recovery assessed; the washed sperm are then kept in culture medium in the incubator for 24 hours and then rechecked. If there are more than 3 million motile sperm per ml, this is reassuring. If, however, none of the sperm is alive after 24 hours, this suggests that they may be functionally incompetent. Treatment depends upon how low the count is. If it is only moderately decreased (total motile sperm count in the ejaculate being 20 million), it makes sense to try to improve the fertility potential of the wife, and the easiest treatment for men with moderately low sperm counts is superovulation plus intrauterine insemination. If after doing this and trying for 4 treatment cycles (the reason 4 is the "magic" number is that most patients who are going to become pregnant with any method will usually do so within 4 cycles) no pregnancy ensues, you need to go on and explore further alternatives, such as IVF or ICSI.
For men with a motile sperm count of more than 5 million in the ejaculate, IVF would be the first treatment offered. This would allow us to document if the sperm can fertilize the eggs or not. If fertilisation is documented, then the patient has a good chance of getting pregnant. However, if the motile sperm count is less than 5 million, or if there is total failure of fertilisation in IVF, then the only treatment available is ICSI (intracytoplasmic sperm injection, pronounced "eeksee") or microinjection. ICSI has revolutionised our approach to the infertile man, and it promises the possibility for every man to have a baby, no matter how low his sperm count.
Why do I have a low sperm count ?
What about the answer to the million dollar question: --- Why do I have a low sperm count? Unfortunately, nine times out of ten, the doctor will not be able to answer that question, and no amount of testing will help us to find out - this is labelled as "idiopathic oligospermia" which is really a wastepaper basket diagnosis for "god only knows!". Modern research has shown that the reason some men have a low sperm count maybe because of a microdeletion on the Y-chromosome. This is an expensive test, which is available only in research laboratories at present, and does explain why we have little effective treatment for this common problem! We do know that a low sperm count is not related to physique, general state of health, diet, sexual appetite or frequency. While not knowing the cause can be very frustrating, medicine still has a lot to study and understand about male infertility, which is a relatively neglected field today.
Is there any connection between a low sperm count and sexual performance ?
The major cause of male infertility usually is a sperm problem. However, do remember that this is no reflection on your libido or sexual prowess. Sometimes men with testicular failure find this difficult to understand (but doctor, I have sex twice a day! How can my sperm count be zero?). The reason for this is that the testis has two compartments. One compartment, the seminiferous tubules, produces sperms. The other compartment, the "interstitium" or the tissue in between the tubules (where the Leydig cells are) produces the male sex hormone, testosterone, which causes the male sexual drive. Now while the tubules can be easily damaged, the Leydig cells are much more resistant to damage, and will continue functioning normally in most patients with testicular failure.
This is why the diagnosis of a low sperm count can be such a blow to one's ego --- it is so totally unexpected, because it is not associated with other symptoms or signs. Men react differently - but common feelings include anger with the wife and the doctor; resentfulness about having to participate in infertility testing and treatment since they feel having babies is the woman's "job"; loss of self-esteem; and temporary sexual dysfunction such as loss of desire and poor erections. Many men also feel very guilty that because of "their" medical problem, they are depriving their wife the pleasures of experiencing motherhood. Unfortunately, social support for the infertile man is practically non-existent, and he is forced to put up a brave front and show that he doesn't care. Since he is a man, he is not allowed to display his emotions. He is expected to provide a shoulder for his wife to cry on - but he needs to learn to cry alone. However, remember that the urge for fatherhood can be biologically as strong as the urge for motherhood - and we should stop treating infertile men as second class citizens.
Why is treatment of a low sperm count so confusing ?
Many infertile men are obsessed about their sperm count - and this seems to become the central concern in their lives. Remember that the real question the man with a fertility problem is asking is not: What is my sperm count or motility or whatever? But - are my sperm capable of working or not? Can I have a baby with my sperm? Since the function of the sperm is to fertilize the egg, the only direct way of answering this question is by actually doing IVF for test fertilization. This is, of course, too expensive and impractical for most people which is why the other sperm function tests have been devised.
The major problem with all these tests, however, is that they are all indirect --- there is no very good correlation between test results, pregnancy rates, and fertilization in vitro for the individual patient. This is why offering a prognosis for the individual patient based on an abnormality in the sperm test result is so difficult, and why we find that different doctors give such widely varying interpretations based on the same sperm report.
This is really not surprising when you consider how abysmal our ignorance in this area is - after all, we do not even know what a "normal" sperm count is! Since you only need one "good" sperm to fertilise an egg, we do not have a simple answer to even this very basic question! While the lower limit of normal is considered to be 10 million progressively motile sperm per ml, remember that this is a statistical average. For example, most doctors have had the experience of a man with a very low sperm count (as little as 2-5 million per ml) fathering a pregnancy on his own, with no treatment. In fact, when sperm counts are done for men who are undergoing a vasectomy for family planning, these men of proven fertility have sperm counts varying anywhere from 2 million to 300 million per ml. This obviously means that there is a significant variation in "fertile" sperm counts, and therefore coming to conclusions is very difficult for the doctor (leave alone the patient!)
In order to make sense of this, you need to understand two important concepts - "trying time" and "fertility potential of the couple". If your sperm count is low, but you have been trying to have a baby for less than 1 year, it still makes sense to keep on trying for about 1 year, since 10% of men with low sperm counts will father a pregnancy in this time. If however, you have already tried for more than 2 years with no success, you need to move on and do something more - the chances of a spontaneous pregnancy are now very low. Remember, that a doctor does not treat just a "low sperm count report" - he treats patients!
What can the man with a low sperm count do ?
So what is the man with a low sperm count to do? Unfortunately, there is no method of increasing the sperm count today! The modern protocol for managing male infertility is based on the man's motile sperm count; and on a simple test, called a sperm survival test. The sperm are washed, and their recovery assessed; the washed sperm are then kept in culture medium in the incubator for 24 hours and then rechecked. If there are more than 3 million motile sperm per ml, this is reassuring. If, however, none of the sperm is alive after 24 hours, this suggests that they may be functionally incompetent. Treatment depends upon how low the count is. If it is only moderately decreased (total motile sperm count in the ejaculate being 20 million), it makes sense to try to improve the fertility potential of the wife, and the easiest treatment for men with moderately low sperm counts is superovulation plus intrauterine insemination. If after doing this and trying for 4 treatment cycles (the reason 4 is the "magic" number is that most patients who are going to become pregnant with any method will usually do so within 4 cycles) no pregnancy ensues, you need to go on and explore further alternatives, such as IVF or ICSI.
For men with a motile sperm count of more than 5 million in the ejaculate, IVF would be the first treatment offered. This would allow us to document if the sperm can fertilize the eggs or not. If fertilisation is documented, then the patient has a good chance of getting pregnant. However, if the motile sperm count is less than 5 million, or if there is total failure of fertilisation in IVF, then the only treatment available is ICSI (intracytoplasmic sperm injection, pronounced "eeksee") or microinjection. ICSI has revolutionised our approach to the infertile man, and it promises the possibility for every man to have a baby, no matter how low his sperm count.
Why do I have a low sperm count ?
What about the answer to the million dollar question: --- Why do I have a low sperm count? Unfortunately, nine times out of ten, the doctor will not be able to answer that question, and no amount of testing will help us to find out - this is labelled as "idiopathic oligospermia" which is really a wastepaper basket diagnosis for "god only knows!". Modern research has shown that the reason some men have a low sperm count maybe because of a microdeletion on the Y-chromosome. This is an expensive test, which is available only in research laboratories at present, and does explain why we have little effective treatment for this common problem! We do know that a low sperm count is not related to physique, general state of health, diet, sexual appetite or frequency. While not knowing the cause can be very frustrating, medicine still has a lot to study and understand about male infertility, which is a relatively neglected field today.
Is there any connection between a low sperm count and sexual performance ?
The major cause of male infertility usually is a sperm problem. However, do remember that this is no reflection on your libido or sexual prowess. Sometimes men with testicular failure find this difficult to understand (but doctor, I have sex twice a day! How can my sperm count be zero?). The reason for this is that the testis has two compartments. One compartment, the seminiferous tubules, produces sperms. The other compartment, the "interstitium" or the tissue in between the tubules (where the Leydig cells are) produces the male sex hormone, testosterone, which causes the male sexual drive. Now while the tubules can be easily damaged, the Leydig cells are much more resistant to damage, and will continue functioning normally in most patients with testicular failure.
This is why the diagnosis of a low sperm count can be such a blow to one's ego --- it is so totally unexpected, because it is not associated with other symptoms or signs. Men react differently - but common feelings include anger with the wife and the doctor; resentfulness about having to participate in infertility testing and treatment since they feel having babies is the woman's "job"; loss of self-esteem; and temporary sexual dysfunction such as loss of desire and poor erections. Many men also feel very guilty that because of "their" medical problem, they are depriving their wife the pleasures of experiencing motherhood. Unfortunately, social support for the infertile man is practically non-existent, and he is forced to put up a brave front and show that he doesn't care. Since he is a man, he is not allowed to display his emotions. He is expected to provide a shoulder for his wife to cry on - but he needs to learn to cry alone. However, remember that the urge for fatherhood can be biologically as strong as the urge for motherhood - and we should stop treating infertile men as second class citizens.
Why is treatment of a low sperm count so confusing ?
Many infertile men are obsessed about their sperm count - and this seems to become the central concern in their lives. Remember that the real question the man with a fertility problem is asking is not: What is my sperm count or motility or whatever? But - are my sperm capable of working or not? Can I have a baby with my sperm? Since the function of the sperm is to fertilize the egg, the only direct way of answering this question is by actually doing IVF for test fertilization. This is, of course, too expensive and impractical for most people which is why the other sperm function tests have been devised.
The major problem with all these tests, however, is that they are all indirect --- there is no very good correlation between test results, pregnancy rates, and fertilization in vitro for the individual patient. This is why offering a prognosis for the individual patient based on an abnormality in the sperm test result is so difficult, and why we find that different doctors give such widely varying interpretations based on the same sperm report.
This is really not surprising when you consider how abysmal our ignorance in this area is - after all, we do not even know what a "normal" sperm count is! Since you only need one "good" sperm to fertilise an egg, we do not have a simple answer to even this very basic question! While the lower limit of normal is considered to be 10 million progressively motile sperm per ml, remember that this is a statistical average. For example, most doctors have had the experience of a man with a very low sperm count (as little as 2-5 million per ml) fathering a pregnancy on his own, with no treatment. In fact, when sperm counts are done for men who are undergoing a vasectomy for family planning, these men of proven fertility have sperm counts varying anywhere from 2 million to 300 million per ml. This obviously means that there is a significant variation in "fertile" sperm counts, and therefore coming to conclusions is very difficult for the doctor (leave alone the patient!)
In order to make sense of this, you need to understand two important concepts "trying time" and "fertility potential of the couple". If your sperm count is low, but you have been trying to have a baby for less than 1 year, it still makes sense to keep on trying for about 1 year, since 10% of men with low sperm counts will father a pregnancy in this time. If however, you have already tried for more than 2 years with no success, you need to move on and do something more - the chances of a spontaneous pregnancy are now very low. Remember, that a doctor does not treat just a "low sperm count report" - he treats patients!
What can the man with a low sperm count do ?
So what is the man with a low sperm count to do? Unfortunately, there is no method of increasing the sperm count today! The modern protocol for managing male infertility is based on the man's motile sperm count; and on a simple test, called a sperm survival test. The sperm are washed, and their recovery assessed; the washed sperm are then kept in culture medium in the incubator for 24 hours and then rechecked. If there are more than 3 million motile sperm per ml, this is reassuring. If, however, none of the sperm is alive after 24 hours, this suggests that they may be functionally incompetent. Treatment depends upon how low the count is. If it is only moderately decreased (total motile sperm count in the ejaculate being 20 million), it makes sense to try to improve the fertility potential of the wife, and the easiest treatment for men with moderately low sperm counts is superovulation plus intrauterine insemination. If after doing this and trying for 4 treatment cycles (the reason 4 is the "magic" number is that most patients who are going to become pregnant with any method will usually do so within 4 cycles) no pregnancy ensues, you need to go on and explore further alternatives, such as IVF or ICSI.
For men with a motile sperm count of more than 5 million in the ejaculate, IVF would be the first treatment offered. This would allow us to document if the sperm can fertilize the eggs or not. If fertilisation is documented, then the patient has a good chance of getting pregnant. However, if the motile sperm count is less than 5 million, or if there is total failure of fertilisation in IVF, then the only treatment available is ICSI (intracytoplasmic sperm injection, pronounced "eeksee") or microinjection. ICSI has revolutionised our approach to the infertile man, and it promises the possibility for every man to have a baby, no matter how low his sperm count.
Why do I have a low sperm count ?
What about the answer to the million dollar question: --- Why do I have a low sperm count? Unfortunately, nine times out of ten, the doctor will not be able to answer that question, and no amount of testing will help us to find out - this is labelled as "idiopathic oligospermia" which is really a wastepaper basket diagnosis for "god only knows!". Modern research has shown that the reason some men have a low sperm count maybe because of a microdeletion on the Y-chromosome. This is an expensive test, which is available only in research laboratories at present, and does explain why we have little effective treatment for this common problem! We do know that a low sperm count is not related to physique, general state of health, diet, sexual appetite or frequency. While not knowing the cause can be very frustrating, medicine still has a lot to study and understand about male infertility, which is a relatively neglected field today.
Is there any connection between a low sperm count and sexual performance ?
The major cause of male infertility usually is a sperm problem. However, do remember that this is no reflection on your libido or sexual prowess. Sometimes men with testicular failure find this difficult to understand (but doctor, I have sex twice a day! How can my sperm count be zero?). The reason for this is that the testis has two compartments. One compartment, the seminiferous tubules, produces sperms. The other compartment, the "interstitium" or the tissue in between the tubules (where the Leydig cells are) produces the male sex hormone, testosterone, which causes the male sexual drive. Now while the tubules can be easily damaged, the Leydig cells are much more resistant to damage, and will continue functioning normally in most patients with testicular failure.
This is why the diagnosis of a low sperm count can be such a blow to one's ego --- it is so totally unexpected, because it is not associated with other symptoms or signs. Men react differently - but common feelings include anger with the wife and the doctor; resentfulness about having to participate in infertility testing and treatment since they feel having babies is the woman's "job"; loss of self-esteem; and temporary sexual dysfunction such as loss of desire and poor erections. Many men also feel very guilty that because of "their" medical problem, they are depriving their wife the pleasures of experiencing motherhood. Unfortunately, social support for the infertile man is practically non-existent, and he is forced to put up a brave front and show that he doesn't care. Since he is a man, he is not allowed to display his emotions. He is expected to provide a shoulder for his wife to cry on - but he needs to learn to cry alone. However, remember that the urge for fatherhood can be biologically as strong as the urge for motherhood - and we should stop treating infertile men as second class citizens.
Microinjection: The Latest Advance in Treating the Infertile Man
The introduction of Microinjection Technology into the in vitro fertilization laboratory has revolutionized our treatment of the infertile man. Intracytoplasmic sperm injection, or ICSI (pronounced "eeksee"), is a new infertility treatment that uses micromanipulation technology for treating male infertility. What ICSI promises is the possibility for every man to father his own baby - no matter what his medical problem!
What exactly is ICSI? As the name suggests, ICSI a technique in which a single sperm is injected into the centre of the cytoplasm of the egg, in order to achieve fertilization . While this may sound very crude, ICSI allows the IVF laboratory to achieve fertilization with very few sperm. The beauty of the technique is that since the sperm is being injected directly into the egg, all that is needed to achieve fertilization are live sperm - no matter how abnormal these may appear to be. With ICSI the equation "1 egg plus 1 sperm = 1 embryo" becomes possible!
The Procedure for ICSI ICSI is done in a superovulated cycle during which fertility drugs (human menopausal gonadotropin - HMG- injections) are administered to the wife to aid in the production of multiple eggs, which are then removed under vaginal ultrasound guidance as is done for IVF.
In normal circumstances, the egg is surrounded by a cluster of cells known as the cumulus corona cells, and this is called the oocyte cumulus corona complex.
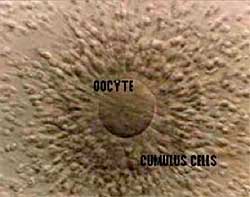
These cumulus cells are removed by repeated passage of the oocyte cumulus corona complex through fine pipettes, and by treating them with a chemical called hyaluronidase so that these cells are stripped off.The denuded eggs are examined, and only mature eggs (eggs in metaphase II, which have a polar body) are used for ICSI.
Sperm is collected from the man, usually through masturbation. For men with severe oligospermia, we have found it useful to use sequential ejaculates. Even though the first semen sample may not contain any sperm, we often find motile sperm in the second ( or even the third sample, for men with enough stamina !) This maybe because the later samples contain "fresher" sperm. Since these samples contain such few sperm, they need to processed very carefully, so that the all the sperm in the sample are recovered in the culture medium , and can be used for ICSI.
For men with variable sperm counts, which vary from zero to a few thousand, it may be helpful to freeze a sample ( which contains sperm ) in advance. For patients with azoospermia, sperm harvesting techniques need to be used to retrieve the sperm. For men with obstructive azoopsermia,( because of duct blockage or absence of the vas deferens) , the simplest technique is called PESA (percutaneous epididymal sperm aspiration), in which the sperm is sucked out from the epididymis by puncturing it with a fine needle. Occasionally, one may have to use microsurgery to find epididymal sperm, and this is called MESA (microepididymal sperm aspiration).
How can ICSI be used to treat men with a zero sperm count ( azoospermia) ?
For patients with obstructive azoopsermia in whom sperm cannot be found in the epididymis, it is always possible to find sperm in the testis. The easiest way to retrieve this is through TESA or testicular sperm aspiration , in which the testicular tissue is sucked out through a fine needle, under local anaesthesia. The testicular tissue is placed in culture media and sent to the lab, where it is processed. The sperm are liberated from within the seminiferous tubules ( where they are produced ) and are then dissected free from the surrounding testicular tissue.
Using sperm from the epididymis and testis for ICSI in order to treat patients with obstructive azoospermia is logical, and thus conceptually easy to understand. However, surprisingly, it is possible to find sperm even in patients who have testicular failure ( nonobstructive azoospermia) - even in those men with very small testes. The reason for this is that defects in sperm production are "patchy"- they do not affect the entire testis uniformly.
This means that even if sperm production is absent in a certain area, there may be other areas in the testis where sperm production would be normal (this could be because the genetic defect that causes abnormal spermatogenesis may be "leaky"). Since such few sperm are needed for ICSI, we can find enough sperm in over 50 per cent of patients with testicular failure , even if their testes are as small as a peanut!
What is TESE ( testicular sperm extraction) ICSI ?
However, while finding sperm is quite easy in men with obstructive azoospermia ( since their testes are functioning normally ), patients with nonobstructive azoospermia ( testicular failure) can be very challenging. Often, sperm production in these men is sparse, and multiple sites in the testis may need to be sampled before being able to find sperm. This can be done by performing mutiple tiny microbiopsies , and this is called TESE or testicular sperm extraction. ( One of our patients suggested that we call this procedure TSEICSI - which stands for testicular sperm extraction with ICSI, and pronounce it as "sexy"!) This can be done through the needle, or as an open procedure performed under direct vision through a tiny skin incision under local anesthesia and sedation.
Finding sperm in the testicular tissue can be a laborious process , depending on the degree of sperm production, and for some men with partial testicular failure, it can take upto 2-3 hours to find the sperm. Also, testicular sperm are technically hard to work with in the laboratory and only some IVF clinics have the requisite expertise. For men with nonobstructive azoopsermia, some clinics perform the TESE the day prior to egg retrieval, because they believe culturing the testicular tissue in the incubator for 24 hours helps the sperm to acquire motility, which makes them easier to work with. In case no sperm are found, either the couple decides to cancel the egg retrieval and abandon the cycle, or to go ahead with using donor sperm for IVF, as a backup option.
In patients in whom surgery needs to be performed in order to recover testicular or epididymal sperm, it is now possible to freeze the excess sperm. These sperm can then be thawed and used in future cycles in needed, thus sparing the patient the need for repeated surgery for sperm retrieval.
How is a single sperm injected into the egg for ICSI in the IVF laboratory ?
Once eggs and sperm have been collected, the actual process of injecting a single sperm into the egg is carried out in a laboratory. The injection is performed on a heating stage, on a specialized inverted microscope (which allows one to magnify details up to 400 times) equipped with Hoffman modulation contrast optics (which enhance "optical contrast", so that the details of the egg can be visualized easily). The precise control that is needed for microinjection is provided by using specialized micromanipulators, which allow one to execute very fine movements.
The eggs and sperm are manipulated using fine glass pipettes, made of thin capillary tubing, which are even finer than a human hair. These are custom made, the holding pipette being designed to hold a single sperm. Live sperm are placed in a drop of viscous polyvinyl pyrrolidone (PVP) solution, which serves to slow down the activity of the sperm. (It is helpful to slow down the sperm, so that they can be picked up more easily by the injecting needle.) A single sperm is then selected and its tail is pinched or broken to immobilize it. This is usually done by crushing the sperm tail by rolling it between the injection pipette and the base of the petri dish. It is essential to immobilize the sperm, so that it cannot move after it has been injected into the egg. A single immobile sperm is then picked up by sucking it into the injection pipette.
The egg is secured in place by applying gentle suction to its shell (the zona) with a holding pipette. The sperm is then injected directly into the centre (cytoplasm) of the egg by moving the injection pipette very precisely with the help by moving the injection pipette very precisely with the help of the micromanipulator into the egg, and then blowing the sperm out very gently into the cytoplasm of the egg. In order to do this, it is important to breach the zona of the egg and the outer membrane of the egg. The skill of the embryologist is a critical factor in the success of the ICSI process. After injecting the sperm, the pipette is withdrawn. Remarkably, once the injecting pipette is withdrawn, the egg will close and assume its original shape within 60 seconds. One can visualize ICSI as the sperm being given a "piggyback" ride into the egg, so that what the sperm cannot accomplish on its own, the laboratory does for it! The only requirement for ICSI is that the sperm should be alive, and there should be as many sperm as there are eggs.

Fig 1. A view of the micromanipulator
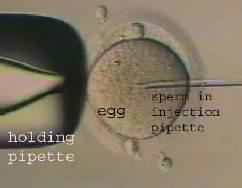
Fig 2. A single sperm is being injected into an egg during an ICSI procedure
Once all the eggs are injected with a single sperm each, they are placed in the CO2 incubator, and then observed approximately 14 hours later to see if fertilization has taken place. If fertilization has occurred, the 2-4 cell embryos can be transferred into the wife?s uterus about 48-72 hours after ICSI, as is done for IVF. Interestingly, embryo implantation rates in these patients are quite high, because the wives are usually young and completely normal.
Fertilization rates in the range of 60-80 per cent have been achieved in experienced hands-which means, of 100 microinjection eggs about 60 form embryos after ICSI . In fact the technology is now reliable enough to virtually guarantee fertilization, if there are sufficient good quality eggs. The pregnancy rate in one ICSI cycle is about 35 percent. Remarkably, the chance of achieving a pregnancy does not depend upon the sperm count or number (since you only need as many sperm as there are eggs!), but rather on the number and quality of eggs retrieved, which, in turn, depend upon the woman?s age. The risk of having a baby with a birth defect is not increased with this technique.
ICSI is expensive at present, because of the advanced technology it utilizes. Nevertheless, it is now available in most of India?s large cities, and as times goes by, it is hoped that the cost of this procedure will decrease, making it affordable for more patients.
ICSI has now become the preferred method of achieving in vitro fertilisation in our clinic. This reduces the risk of unexpected total fertilisation failure sometimes seen with IVF ( research has shown that up to 25% of patients with "unexplained " infertility with an apparently normal semen analysis may have dysfunctional sperm which cannot fertilise eggs in vitro).
What are the risks of doing ICSI ?
The Risk Factor
More than 100,000 babies have been born worldwide after ICSI , and detailed studies have shown that there is no increased risk of birth defects or genetic anomalies , as a result of the technique.
It is possible , however, that some of the male children born as a result of this technique may be infertile as well (for example, if the cause for the testicular failure is a defective genetic locus, such as a microdeletion on the Y chromosome).
What recent advances have taken place in ICSI ?
Recent Advances
For some patients with severe testicular failure, sometimes, it is not possible to find any sperm at all as even in spite of taking multiple testicular biopsies. In such patients pregnancies have been achieved even by injecting round spermatids (immature precursor cells from which the sperm are formed) from the testis into the egg. This is now an area of intense research all over the world, but the results have been disappointing so far. Other labs are trying to develop methods of in vitro spermatogenesis, in order to mature the spermatids in vitro.
For men with no testis at all, the only technologic solution today would be cloning using nuclear transfer technology. This involves inserting the nucleus from an ordinary cell of the man ( which contains all his DNA) into his wife?s unfertilised egg (the nucleus of which has been removed) and then activating it by electrofusion. While cloning has been performed successfully in many animal species, it has never been used for treating humans so far.
AUTHOR
SESAN SAMUEL OYEDEPO
Article Source: http://www.articlesbase.com/men%27s-health-articles/the-man-with-a-low-sperm-count-cause-treatment-966727.html